Emiliano Pablo Ravera and Adam Rozumalski
Gait & Posture
Introduction: Spasticity in children with cerebral palsy (CP) can produce an increase in muscle activity with unknown consequences in muscle energy expenditure. Selective dorsal rhizotomy (SDR) is shown to significantly reduce spasticity [Chen2019]. However, Zaino et al. (2020) showed that changes in energy consumption following SDR are not significantly different from matched controls with CP.
Research Question: Can individual muscle energy expenditure be altered after SDR during walking?
Retrospectively, two groups of individuals younger than 14, with a primary diagnosis of bilateral spastic CP, who underwent gait analysis at Gillette Children’s Specialty Healthcare between 1994 and 2020 were identified. The first group (treatment) consisted of individuals who: 1) underwent a bilateral SDR before the age of 12 years, 2) had at least one gait analysis before (baseline) and after (follow-up) SDR. The second group (control) matched the first but did not undergo SDR.
Methods: These groups were matched on baseline levels of age, weight, spasticity, energy consumption, non dimensional walking speed, GDI and follow-up levels of age, weight and non-dimensional walking speed. The Designmatch R-package was used to match the groups. All matching parameters were compared between groups to evaluate similarity of the cohorts using Wilcoxon test (α=0.05). Neuro-musculoskeletal simulations from EMG-informed models using OpenSim were performed. Simulations for 3-8 walking trials were generated for each subject. The model was a simplified version of the gait2392 model [Delp1990]. The scaled model was morphologically adjusted to pediatric participants with CP by using validated techniques. The muscle energy expenditure was computed following Umberger et al. (2003). The difference between the mean of muscle energy expenditure during gait at baseline and follow-up for both groups was calculated.
Results: A total of 81 individuals with CP (45 male, 36 female) who underwent an SDR were identified for the treatment group (age 6y 7mo [3y 7mo, 11y 2mo]; height 116cm [96.5cm, 157cm]; weight 22.4Kg [13.2kg, 63.1Kg]). The control group consisted of 81 individuals with CP (50 males, 31 females) who did not undergo SDR (age 6y 7.3mo [3y 8mo, 11y 3mo]; height 115.9cm [94cm, 139cm]; weight 21.8Kg [12.7kg, 41.6Kg]). There were no statistical differences between groups for all matched
parameters. Vastus and gluteus maximus were the only two muscles simulated that did not have a significant difference in muscle alterations between the two groups [Figure 1]. Soleus and semimembranosus in the control group were the only two muscles to retain their forces from baseline.
Discussion: The results of the modeling show that significantly more calf force can be maintained after SDR than after other treatments. As this is an important muscle for both propulsion and support, it may help explain the differences seen in the current outcomes’ literature.
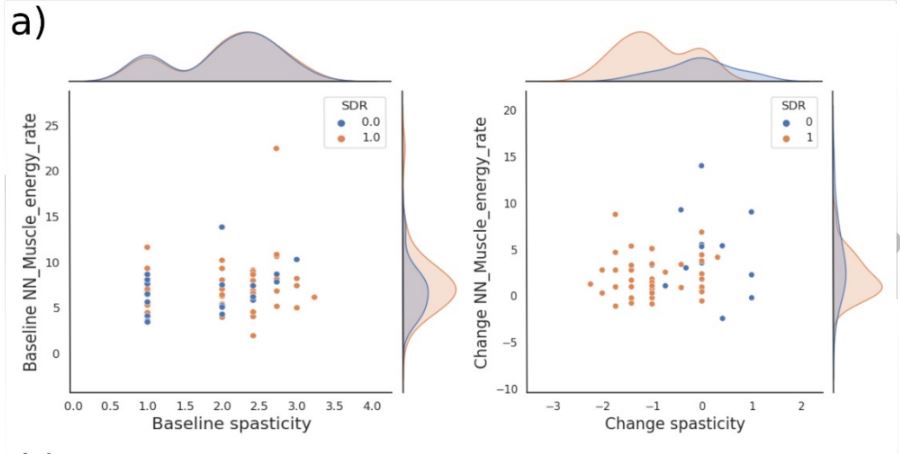
Fig. 1.a) Spasticity and net-nondimensionalized (NN) total muscle energy expenditure for both groups.